




Over the last dozen years or so, many pediatricians, astounded by the ramifications of the science of adverse childhood experiences (ACEs) on the children they care for, began integrating this science into their practices.
The most common approach has been to ask parents about ACEs using a questionnaire, and to use this information to counsel parents and identify resources for the family. Different practices have been using different questionnaires: Some ask parents for their ACE scores along with their children’s; others also add a resilience survey.

As a physician AND a researcher, Dr. Ariane Marie-Mitchell took a slightly different approach: She began walking a methodical path to provide basic clinical research to help translate the science of adversity and resilience into practice. And, of course, as any pioneer, she slammed into a few obstacles along the way.
The short version is that now, nine years after Marie-Mitchell first learned about the CDC-Kaiser Permanente Adverse Childhood Experiences Study, all children at Loma Linda University’s resident clinic in Loma Linda, CA, are being screened for childhood adversity. About 2,000 kids have been screened so far, and they and their families are being provided resources. In addition, every year, about 70 medical residents from Loma Linda University Health learn about ACEs science, and there’s so much buzz about ACEs science that several residents are starting research projects with Marie-Mitchell.
All the work has been worth it, says Marie-Mitchell: Integrating ACEs science into pediatric practice “has tremendous power to change the course of someone’s life, if that identification of risk factors is combined with getting the child, family or both the kind of help that they need.”
Here’s the long version of this journey: It began seven years ago, when Marie-Mitchell asked a really basic question in her first research project: Will parents’ reports of their kids ’ childhood adversity actually identify those at risk for developing problems? She did the research as part of an American Academy of Pediatrics Young Investigator award in 2010, when she was working at a clinic in Rochester, NY. Her goal was to test a tool that could be used in a pediatric practice. She asked parents of four- and five-year-olds to fill out a modified ACE survey about their children. She found that the screener identified kids at risk for behavioral problems, developmental delays and injuries. The study — “Adverse childhood experiences: translating knowledge into identification of children at high risk for poor outcomes“ — was published in the journal Academic Pediatrics in 2013.
’ childhood adversity actually identify those at risk for developing problems? She did the research as part of an American Academy of Pediatrics Young Investigator award in 2010, when she was working at a clinic in Rochester, NY. Her goal was to test a tool that could be used in a pediatric practice. She asked parents of four- and five-year-olds to fill out a modified ACE survey about their children. She found that the screener identified kids at risk for behavioral problems, developmental delays and injuries. The study — “Adverse childhood experiences: translating knowledge into identification of children at high risk for poor outcomes“ — was published in the journal Academic Pediatrics in 2013.
In 2011, Marie-Mitchell took a position as assistant professor in the Department of Preventive Medicine and Pediatrics at Loma Linda University Health. To take her research to the next level — actually integrating a survey into a pediatric practice — she began doing focus groups and interviews with parents, pediatricians and their staff, and mental health professionals at two Loma Linda clinics. She wanted to know how to best word questions about ACEs to increase identification of risk factors and to provide community referrals without negatively affecting visit time or patient satisfaction. She also talked with other pediatricians and researchers around the U.S. about how they were implementing ACEs assessments and screening.
In the spring of 2014, she began trying out different wordings of the questions. Using the 10 questions from the original CDC-Kaiser Permanente Adverse Childhood Experiences Study (ACE Study) in a pediatric practice is, well, complicated, says Marie-Mitchell. That’s because the original survey is designed to be taken by adults who identify experiences that happened to them in their childhoods, up to the age of 18. The original survey is not designed for parents or teens who may be concerned about child protective service reports; it’s also not designed to distinguish current trauma from past ACEs.
The ACE Study looked at 10 types of childhood trauma: physical, emotional and sexual abuse; physical and emotional neglect; living with a family member who’s addicted to alcohol or other substances or who’s depressed or has other mental illnesses; experiencing parental divorce or separation; having a family member who’s incarcerated, and witnessing a mother being abused. (Of course, there are other types of adversity, and other subsequent ACE surveys include racism, witnessing violence outside the home, bullying, losing a parent to deportation, living in an unsafe neighborhood, and involvement with the foster care system.)
Pediatricians want to integrate ACE surveys into their practices because of the compelling findings from the ACE Study, which determined that the higher someone’s ACE score – the more types of childhood adversity a person experienced – the higher their risk of chronic disease, mental illness, violence, being a victim of violence and a bunch of other consequences. The study found that most people (64%) have an ACE score of one; 12% of the population has an ACE score of 4. Having an ACE score of 4 nearly doubles the risk of heart disease and cancer. It increases the likelihood of becoming an alcoholic by 700 percent and the risk of attempted suicide by 1200 percent. (For more information, go to ACEs Science 101. To calculate your ACE and resilience scores, go to: Got Your ACE Score?)
The ACE Study also found that it didn’t matter what the types of ACEs were. An ACE score of 4 that included divorce, physical abuse, an incarcerated family member and a depressed family member had the same statistical health consequences as an ACE score of 4 that included living with an alcoholic, verbal abuse, emotional neglect and physical neglect.
The ACE Study is one of five parts of ACEs science, which also includes how toxic stress from ACEs damage children’s developing brains; how toxic stress from ACEs cause chronic diseases; and how it can affect our genes and be passed from one generation to another (epigenetics); and resilience research, which shows the brain is plastic and the body wants to heal. Resilience research focuses on what happens when organizations and systems integrate trauma-informed and resilience-building practices, for example in education and in the family court system.
Asking about children’s ACEs isn’t as simple as asking adults about their past ACEs. “In the pediatric world,” says Marie-Mitchell, “we’re in real time, so it’s more complicated. Do I want to ask what already happened to the child? Do I want to ask what might happen to the child? In this questionnaire, we’re doing both.”
For example, a parent might report that their child is living with a family member who’s experienced substance abuse. The pediatrician wants to know: Is the kid living with a parent who’s abusing alcohol now? Or did it happen a while ago? The answers to both of those questions are important, and the responses are different. If the child is living with a family member who’s abusing alcohol or other drugs now, then the safety of the child’s environment needs to be assessed, and that family member may need a referral for substance abuse treatment programs. If the child lived with a family member who was — but no longer is — abusing alcohol or other drugs, then the pediatrician can assess how that affected the child and the way the family coped.
She received approval from the local Medi-Cal provider to test questions about ACEs on the Staying Healthy Assessment used in the Loma Linda resident clinic. She began testing it in January 2015 on a small group of patients, with successful results. But when the clinic was ready to adopt the new form for all patients, the process slammed into a bureaucratic wall. The state of California requires all pediatricians serving Medi-Cal patients to use its Staying Healthy Assessment or an approved alternative, and hers wasn’t. This meant that Marie-Mitchell had to submit an application and wait for the state to approve her “alternative IHEBA (Individual Health Education Behavioral Assessment)”.

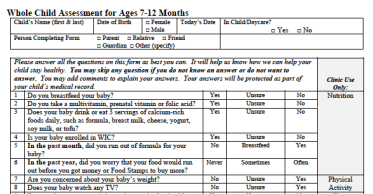
She received final approval for what she calls the Whole Child Assessment (WCA) from the state in October 2016, and began using the integrated assessment with all children in the clinic that serves low-income families in December 2016. This is the clinic where residents from Loma Linda University Medical School work, and where Marie-Mitchell teaches them about how ACEs science helps pediatricians expand a traditional flat-medical approach to a holistic approach to children’s health that captures more aspects of their lives that affect their health.
And now that the WCA is approved, any pediatrician in California who sees Medi-Cal patients can use it. “The WCA tries to improve sensitivity through multiple questions and answer choices, as well as integration of questions about ACEs into a whole child evaluation by age group,” Marie-Mitchell wrote in a post on ACEs Connection. “If you are a California physician and would like to use the WCA, then you may make this request through your local managed care plan and, since the WCA has already been approved by the state, the process should be quite simple. If you are serving non-Medicaid patients or practicing outside of California, you have the option of using the WCA in its current form, or modifying it to fit your practice.”
The WCA comprises several versions for different age groups: 0-6 months, 7-12 months, 1-2 years, 3-4 years, 5-8 years, and 9-11 years. All these are filled out by parents or caregivers. Another version for 12-17 year-olds is filled out by the kids themselves. Each version has about 50 questions that cover ACEs, nutrition, physical activity, safety of the environment in which the child lives and travels, and experiences at school. (Spanish and English versions of the WCA are attached to this post for download.)
“One thing I liked about what we’re doing that’s not necessarily what other folks are doing,” says Marie-Mitchell, “is that our ACEs questions are built into a lifestyle assessment. It normalizes the questions when you’re asking about fruits and veggies, seatbelt use, domestic violence all at the same time. These are behaviors that happen that we need to know about to protect a child’s health.”
Some pediatric practices ask parents about their ACEs, too, and Marie-Mitchell did the same at the start of the project. “We ended up taking them off,” she says. “We weren’t quite sure how useful these questions would be for the child’s experience. I would argue it would be useful.” But it adds to the complexity, she says. If a parent indicates she or he was sexually abused, for example, “it doesn’t matter if it happened 50 years ago, that provider is obligated to report that if the abuser is still alive and has children in their custody,” she says.
Nevertheless, all parents and caregivers are educated about ACEs science. If the parents or caregivers indicate that their child has experienced adversity, then the residents may ask open-ended questions, such as: “I see that you have had these challenges; how can we be helpful to you?” And then they integrate information about ACEs science into the conversation.
So far, Marie-Mitchell believes that integrating the ACEs questions as part of a whole child assessment has been useful for physicians and parents. For example, residents learn how food insecurity can be a risk factor for child neglect, and can use information gleaned from the survey to connect parents and caregivers to food pantries and, if their children are under the age of five, get parents enrolled in the USDA’s Women, Infants and Children nutrition program (WIC).
“I also think it’s affirming for the parent to know that this an important part of what is relevant to the doctor to know about what is going on with the child,” she says. “It improves the doctor/patient relationship by improving the parent’s perception about how the pediatrician is approaching the care of their child.”
Because the clinic is part of a Federally Qualified Health Center, parents have immediate access to a family resource center and community resource advocates who can provide assistance if issues are identified during screening, explains Marie-Mitchell. “There are also behavioral health providers — social workers and counselors in the same building,” she says.
 Marie-Mitchell is completing this first phase of research, which is “simply to validate the accuracy of our screening tool,” she notes. “As part of this research we are examining questions about resilience to add to our clinic screening. Next steps for our research include looking at differences in risk factor identification by age group, examining the impact of trauma-informed organizational changes on risk factor reporting, and testing interventions that can improve outcomes for children with ACEs.”
Marie-Mitchell is completing this first phase of research, which is “simply to validate the accuracy of our screening tool,” she notes. “As part of this research we are examining questions about resilience to add to our clinic screening. Next steps for our research include looking at differences in risk factor identification by age group, examining the impact of trauma-informed organizational changes on risk factor reporting, and testing interventions that can improve outcomes for children with ACEs.”
She’s also working with Dr. Brian Distelberg, who’s developed a comprehensive resilience questionnaire, to assess resilience of the parents/caregivers, their children and the communities in which they live. “We want to know which resilience questions change the relationship that we see with high ACEs and their outcomes, so that we can figure out which resilience questions to include in the assessment we use in the clinic,” says Marie-Mitchell.
At some point, a clinically tested version 2.0 of the Whole Child Assessment will be developed based on their research data and clinical experience. The revision may include questions for parents, resilience questions, as well as questions about other types of ACEs, such as neighborhood violence, racism and involvement with the foster care system that other pediatricians — including Nadine Burke Harris at the Center for Youth Wellness in San Francisco, CA, RJ Gillespie at Children’s Clinic in Portland, OR, and Meredith Kieschnick at Roseland Pediatrics in Santa Rosa, CA — have included in their assessments.
Last month, Marie-Mitchell did a presentation for the faculty at Loma Linda University Health about how the assessment is working in the clinic. Since most of the faculty at Loma Linda don’t see Medi-Cal patients, they don’t need to use the state-approved 50-question assessment. They expressed interest in a shorter questionnaire, which is being developed.
Marie-Mitchell’s research and clinical work have become the pebbles in the pond that have led to ripples of activity in San Bernardino and Riverside counties. Last year, she launched the ACEs Task Force of San Bernardino County. This group has developed a brief assessment of trauma-informed organizations and is putting together a resource list for pediatric practices and others in the county. She is also working with the Riverside County Public Health Department to launch a resilience initiative through several clinics in the county.
And as a result of the state approving the WCA, Marie-Mitchell was invited to participate in a state task force put together by the Managed Care Quality Division of the California Department of Health Care Services to review and update the Staying Healthy Assessment, to remove questions that aren’t relevant, and to include questions that address childhood adversity.
Here is the WCA-Spanish, and WCA.
Ariane Marie-Mitchell (r) and Teri Barila (l), co-founder of Children’s Resilience Initiative in Walla Walla, CA, during panel at ACEs summit in San Francisco October 2016.
Written By Jane Ellen Stevens
Pediatrician develops whole-child assessment tool that includes ACEs questions was originally published @ Jane Ellen Stevens – ACEs Too High and has been syndicated with permission.
Our authors want to hear from you! Click to leave a comment
Related Posts
